
Selection and Rational Use of Stapler in Gastrointestinal Operation
Chen Lin is knowledgeable
In recent years, the advancement of surgical instruments has greatly promoted the development of modern surgery. In the field of gastrointestinal surgery, the emergence and popularization of staplers have raised gastrointestinal anastomosis to a new stage. Compared with traditional manual suture, the application of staplers The digestive tract reconstruction performed can significantly shorten the operation time, greatly reduce tissue damage and bleeding, thereby reducing the average length of hospitalization “At present, more and more surgeons prefer to choose mechanical anastomosis in clinical work. However, anastomosis in gastrointestinal surgery As one of the three major factors affecting gastrointestinal anastomosis, the surgeon itself plays a vital role in the selection of the stapler and the grasp of the operation technique, and the success of the anastomosis is also related to it. Closely related 2 This article will talk about my own views on the selection and rational use of staplers in common surgical procedures for gastric and colorectal surgery.
1. Classification of staplers
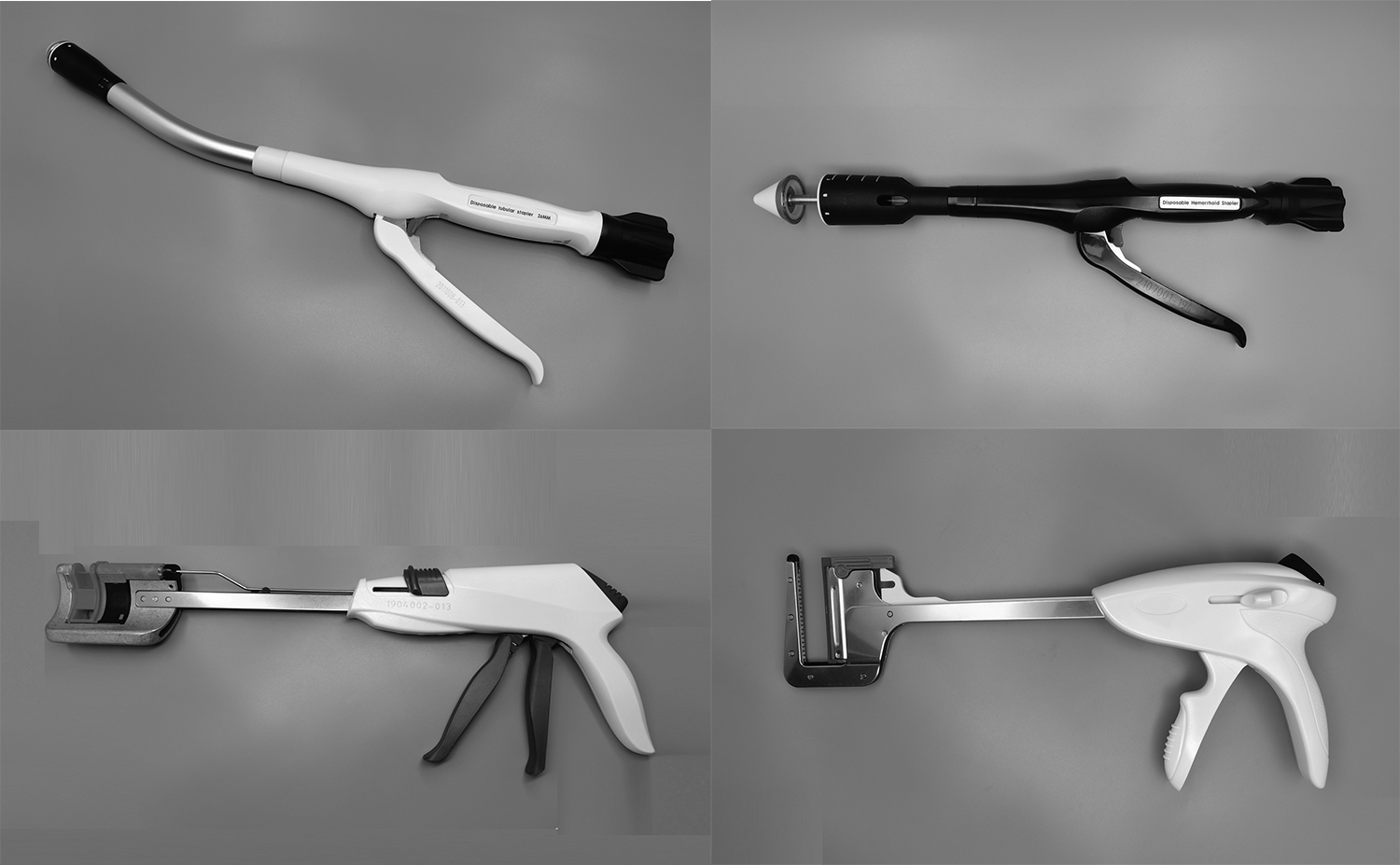
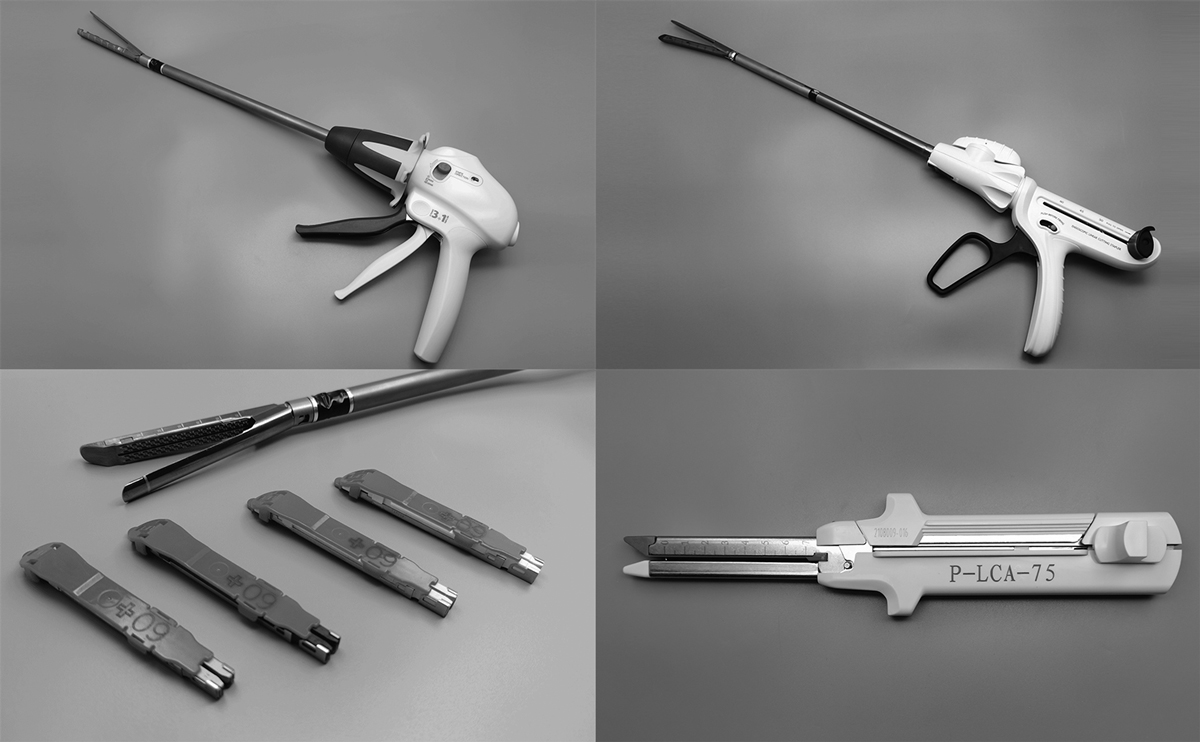
There are many kinds of staplers, which can be divided into press-fit type and staple-type according to the working principle. According to the shape of the stapler, it can be divided into straight-cut stapler, circular-cut stapler, arc-cut stapler, button-shaped stapler and paperclip-shaped stapler.
2. The use of staplers in laparotomy
(1) Selection and application of staplers in gastric surgery
1. Proximal gastrectomy: Circular stapler (CDH25) is generally used for esophagogastric anastomosis, and linear cutting stapler (TLC10) is used for gastric anastomosis. Studies have shown that the use of 25mm stapler for esophagus and gastrointestinal anastomosis can Reduce the occurrence of postoperative complications 3 But this is not absolute. The operator must determine the type of stapler according to the inner diameter of the esophagus. Tissue shaping to reduce anastomotic bleeding Do not pull hard when the stapler withdraws, especially when the incision is incomplete, it may easily cause anastomotic tissue avulsion.
Due to the deep anatomical position of the esophagus, the intraoperative visual field is poor, the anastomosis is difficult, the broken end of the esophagus is easy to tear off, and the incidence of anastomotic leakage is high. However, this has been controversial. Theoretically, suture reinforcement can make the anastomosis more complete and reduce the occurrence of postoperative anastomotic leakage. Easy to form anastomotic stenosis The author’s experience is that the choice should be made according to the anastomotic situation during the operation. If the visual field is clear during the anastomosis, the esophagus is free, the hemostasis is complete, and the anastomotic effect is satisfactory, suture reinforcement is not required; if anastomotic incompleteness or anastomotic bleeding is found during the operation, Seromuscular layer suture can be used to reinforce the suture. Generally, absorbable suture (type 3-0 or 4-0) is selected. Because of the high incidence of foreign body reaction in silk anastomosis, it is easy to form ulcer edema and bleeding at the anastomosis[4] Silk thread, either 3-0 or 1-gauge wire can be used
Although gastric reflux occurs from time to time after esophagogastric anastomosis, which affects the quality of life of patients, but most patients have no obvious symptoms, so this operation is still often used in clinical practice[5]
2. Distal gastrectomy: Bi-type gastroduodenal end-to-side or end-to-end anastomosis Bi-type II gastrojejunostomy and Roux-en-Y gastrojejunostomy are mainly used.
In the Bi I type, circular stapler (CDH25) and linear cutting stapler (TLC10) are used for anastomosis. Some scholars suggest end-to-end anastomosis of gastroduodenum, so that the tension of the anastomosis is small[6] If the tension of the anastomosis is too The risk of postoperative anastomotic leakage will increase [7] The author believes that although the operation of end-to-end anastomosis is complicated, as long as sufficient blood supply and tension-free anastomosis are ensured, the incidence of postoperative complications of the two anastomotic methods is the same. No significant difference.
In the Bi II type, the circular stapler (CDH25) is generally used for anastomosis, and the linear cutting stapler can also be used. The author is used to using the latter to complete the gastrojejunum anastomosis. The endoscopic linear cutting stapler (6TB45) can be used to cut the duodenum. The stapler has a total of 6 rows of staples, and the suture hemostasis function is good, and it is not easy to form duodenal stump fistula and bleeding after operation. If the duodenal stump is edematous, manual suture can be used, and then 6TB45 can be used to complete the gastrojejunal side For lateral anastomosis, attention should be paid to the mesenteric border of the jejunum and the gastric wall of the remnant stomach. Do not bring the mesenteric tissue into the anastomosis. For complications after type II anastomosis, side-to-side jejunum anastomosis (Braun anastomosis) can be added on this basis. After type III anastomosis, alkaline reflux gastritis and anastomotic stomatitis are often prone to occur, so the author uses Bi-I or Roux-en-Y anastomosis.
Gastrojejunum Roux-en-Y anastomosis can use two circular staplers (CDH25) to complete the anastomosis between the jejunum and the gastrojejunum, or use a linear cutting stapler to perform side-to-side anastomosis of the distal jejunum and the remnant stomach through the front of the colon. Note that the direction of the distal jejunum stump is upward, and the direction of the proximal jejunum stump should also be upward during the side-to-side anastomosis of the jejunum. The mesenteric tear at the broken end of the jejunum can be closed with 3-0 silk suture.
3. Total gastrectomy: Esophagojejunostomy, jejunum replacement of stomach, colon replacement of stomach and esophagojejunum Roux-en-Y? Severe, poor quality of life of patients Gastric replacement can significantly improve the quality of life of patients, but the surgical operation is complex Esophagus-jejunum Roux-en-Y anastomosis is moderately difficult and can improve reflux symptoms To choose a suitable reconstruction method, the author recommends Roux-en-Y anastomosis of the esophagus and jejunum. The circular stapler (CDH25) can be used to complete the end-to-side anastomosis of the anterior esophagus and jejunum, and the linear cutting stapler (such as 6TB45) can be used to complete the side-to-side anastomosis of the proximal and distal jejunum. The jejunum stump was closed with 6TB45.
The application of circular staplers in gastrojejunostomy and esophagojejunostomy has been widely accepted, and most surgeons prefer to use circular staplers in open surgery [8-9] Inaba et al.! It is reported that the effect of gastrojejunal anastomosis using linear stapler under laparoscopy is good. The author prefers linear stapler or even stapler under laparoscopic surgery for digestive tract reconstruction in laparotomy.
because:
(1) This type of device is convenient and simple to operate, avoiding the cumbersome operation steps such as the insertion of the purse string suture anvil and the circular stapler passing through the intestinal cavity;
(2) The anastomosis is not limited by the lumen diameter;
(3) There is less bleeding during the anastomosis, and it is not easy to cause tissue tear damage or incomplete anastomosis during anastomosis;
(4) Shorten the operation time:
(5) Compared with the circular stapler, the linear stapler only needs to replace the staple cartridge when it is used multiple times during the operation, which reduces the operation cost. Compared with the circular stapler, whether it can reduce the incidence of postoperative complications, Further clinical validation is yet to be done.
(2) Selection and application of staplers in colorectal surgery
1. End-to-side anastomosis of the ileocolon after right hemicolectomy: a circular stapler (CDH29 or 33) can be used to complete the end-to-side anastomosis of the ileocolon, and a straight line closure (TL60 or TLC75) can also be used to close the stump of the transverse colon. (TLC75) Side-to-side anastomosis of the transverse colon of the ileum In the end-to-side anastomosis between the transverse colon or left hemicolectomy colon, a circular stapler (CDH29 or 33) should be placed in the proximal intestinal lumen.
2. End-to-end anastomosis of colorectum (anal canal) after sigmoid or rectal resection: double anastomosis technique is the most commonly used method in both laparotomy and laparoscopic reconstruction of the digestive tract [11] here mainly introduces double anastomosis Transanal approach for digestive tract reconstruction.
The proximal intestinal canal is placed in a circular stapler anvil, and the distal pre-cut of the tumor is closed with a straight or arc-shaped cutting stapler. The front end of the stapler should be coated with iodine solution before being sent into the anal canal for lubrication and disinfection. The body of the device must be slowly advanced in the anal canal until the front end of the device gently touches the inner side of the rectal stump.
Note: (1) During the tightening of the stapler, prevent the proximal intestine from twisting, otherwise the mesangial vessels will be compressed:
(2) The mesentery at both ends of the anastomosis should not be free too long to ensure sufficient blood supply to the intestine;
(3) The adipose tissue at both ends of the intestinal tube at the anastomosis should be removed to prevent incomplete anastomosis caused by too much tissue embedded during the anastomosis, but it is best not to exceed the range of 2cm, otherwise it will affect the blood supply of the intestinal tube at the anastomosis;
(4) During anastomosis, it is necessary to prevent other irrelevant tissues from being embedded into the stapler, especially the posterior vaginal wall of female patients. The position of the posterior vaginal wall should be confirmed before the stapler is fired, and the vaginal exploration can be performed after the anastomosis is completed;
(5) After the anastomosis is completed, it is best to check whether the anastomosis is complete by “inflating test” or injecting methylene blue solution through the anus, and check the anastomosis by digital examination after operation.
During anastomosis, the overlapping of circular and linear stapler anastomotic lines should be avoided, otherwise the blood supply at the anastomosis will be poor, and anastomotic leakage will easily occur after operation. When using high-frequency electric knife, avoid damage to the rectum and vaginal wall. Although it is widely used, there are still some defects. For example, the staple line of the circular stapler and the linear stapler are easy to overlap during the operation[12]. It is the multiple application of the linear cutting closure during the operation, which will cause the overlap of the anastomotic line and increase the risk of anastomotic leakage[13]. Both the stump and the distal rectum were sutured by purse strings, which can avoid the disadvantages of the double anastomosis technique.
3. Rectal resection and colorectal (anal canal) end-to-side anastomosis: The stapler body can be completed through the abdominal or anal approach. The significance of using circular stapler (CDH33 or 29) and linear stapler It forms a “J”-shaped loop of the colon, which increases the feces storage capacity of the rectum and reduces the risk of postoperative anastomotic leakage. Brisinda et al. [16] found that end-to-side anastomosis is safe and feasible. The incidence of anastomotic leakage is lower, but the sample size of this test is too small, and large-scale clinical trials are still needed for verification.
Colonic pouch-rectal (anal canal) anastomosis can also be used, using a linear cutting stapler to make a 6-7cm J-fold at the free colon end and placing a circular stapler (CDH29 or 33) on the top to anchor the nail A meta-analysis showed that, compared with end-to-side anastomosis, there was no statistically significant difference in postoperative complication rate, mortality, and defecation function between the colonic pouch [15], but the operation of the colonic pouch was complicated and costly It is up to the surgeon to decide which method to choose.
In recent years, curved cutting staplers have gradually become popular in clinical practice. Some scholars believe that in the resection of low rectal cancer, curved staplers are easier to penetrate into the pelvic cavity than linear staplers, and the anastomotic effect is better[16]. Each type of stapler has its own characteristics and indications. For patients with pelvic stenosis and tumors that are located in a low position and whose distal intestinal tract cannot be cut enough with a linear stapler, an arc-cutting stapler may be considered. No matter which stapler you choose, you must The principle of TME should be followed, the anatomy should be clear during the operation, and a good surgical field of view should be ensured.
3. The use of staplers in laparoscopic and da Vinci robotic surgery
1. Gastrointestinal reconstruction of laparoscopic gastrointestinal surgery: divided into complete laparoscopic digestive tract reconstruction, small incision assisted digestive tract reconstruction and hand-assisted laparoscopic digestive tract reconstruction. Complete laparoscopic operation uses various linear cutting staplers and staplers Or circular stapler complete laparoscopic anastomosis with small surgical incision and clear field of vision for patients with quick recovery, but due to the narrow operating space, high technical requirements for the surgeon, high surgical cost, and currently there is no standard surgical method to obtain The clinically recognized small incision-assisted operation is to drag the tissue to be anastomotic out of the abdominal cavity, complete the reconstruction in vitro or insert a stapler under the assistance of a small incision for anastomosis. The operation method is similar to that of laparotomy. Currently, hand-assisted laparoscopy is widely used. Digestive tract reconstruction is to extend the hand into the abdominal cavity through a small incision in the abdominal wall to assist in the anastomosis operation. However, the hand in the abdominal cavity often affects the field of view of the laparoscopic operation, and the anastomotic effect is poor, so it is rarely used.
2. Digestive canal reconstruction in da Vinci robotic gastrointestinal surgery: same as traditional laparoscopic surgery for alimentary canal reconstruction, it can be divided into small incision assisted and full laparoscopic anastomosis.
4. Precautions for reasonable application of stapler:
Although the stapler has brought various conveniences to clinicians, there are still serious postoperative complications that seriously affect the normal function of the gastrointestinal tract [17] Anastomotic leakage, anastomotic stenosis and anastomotic bleeding are relatively common Postoperative complications In order to reduce the incidence of complications, the author believes that the following points should be paid attention to:
(1) The operator must be proficient in the working principle and use method of the stapler, and strictly follow the normal operation steps;
(2) During the operation, it is necessary to carefully check whether the anastomotic anastomosis is complete, whether the ring is complete, and whether there is slight bleeding at the anastomotic site. Once an incomplete anastomosis is found, it should be repaired by manual suture immediately or the original anastomotic intestinal segment should be excised for another reconstruction of the digestive tract. At this time, don’t take chances. When performing manual anastomosis, the author generally uses double-layer interrupted suture method. Although the operation time of single-layer suture method is simple and the operation time is short High strength, not easy to form anastomotic leakage Continuous suture method is easy to form anastomotic stenosis after continuous suture, so interrupted suture is used;
(3) The appropriate stapler must be selected according to the size of the organ and the physiological condition of the patient. Before using the stapler, it must be confirmed that it is intact and there are no missing staples or missing parts;
(4) The surgeon must master the most fundamental operation technique of manual suturing, because some situations may not be suitable for mechanical anastomosis;
(5) Ensure that there is no tension at the anastomosis and the blood supply is good. At the same time, the blood vessels at the mesenteric border of the vessels around the anastomosis should be fully ligated, otherwise postoperative bleeding will easily occur;
(6) The failure of stapler anastomosis often occurs in the anastomosis of esophagus and stomach or small intestine and low rectal anastomosis. Most of them are due to poor visual field and narrow operation space during operation. Therefore, clear dissection, accurate resection and sufficient hemostasis must be performed during operation. , the suture is firm.
At present, staplers can complete almost all gastrointestinal anastomoses, and the latest meta-analysis also shows that in the digestive tract reconstruction of gastrointestinal surgery, mechanical anastomosis has advantages that cannot be compared with manual suture[18], but mechanical anastomosis is only a gastric anastomosis One of the methods of intestinal anastomosis cannot completely replace manual suturing. Only by following the basic principles of surgery and mastering standardized operating steps can clinicians obtain satisfactory surgical results and benefit patients.
Source: Baidu Library
Related ProductsPost time: Jan-12-2023



